
Division of Neuropsychology
Research topics
Research methods
• Apraxia

Spatial neglect is a possible
consequence of right-hemisphere brain damage and is characterised by a
dramatic failure to orient toward, explore and respond to stimuli
presented on the contralesional side, even when these items appear in
isolation or for sustained periods of time. For example, neglect
patients often only talk to people on their right and fail to eat food
from the left side of their plate. Interestingly, while neglect
patients fail to respond to certain regions of space, primary sensory
loss is not the main cause of neglect. In other words, neglect
represents a failure to perceive despite intact sensory processing. In
this lab we study the causal mechanisms and neural basis of this
neuropsychological syndrome using functional MRI, TMS and behavioural
studies in both neurological healthy subjects and neurological
patients.

 |
 |
 |
 |
- Karnath H-O
(2015). Spatial
attention systems in spatial neglect. Neuropsychologia
75: 61-73.
- Li D, Rorden C, Karnath H-O (2017). ‘Nonspatial’ attentional deficits interact with spatial position in neglect. J Cog Neurosci: in press.
- Li D, Rorden C, Karnath H-O (2017). ‘Nonspatial’ attentional deficits interact with spatial position in neglect. J Cog Neurosci: in press.
Classical theories of selective
attention have assumed a single focus of attention. In everyday life,
however, we are more typically confronted with rapidly changing dynamic
scenes that require us to attend simultaneously to multiple
non-contiguous spatial locations (for example traffic scenes). The
importance of this ability to simultaneously attend to multiple spatial
locations is dramatically illustrated in neurological patients
suffering from extinction. Extinction is a common consequence of
unilateral, most frequently right hemispheric brain damage where
patients are able to detect both ipsi- and contralesional information
presented in isolation, but are unable to attend and respond to
contralesional information in situations where ipsilesional information
is concurrently present. Using a combination of fMRI, TMS,
lesion-symptom mapping and psychophysical methods in neurologically
healthy subjects and neuropsychological patients, we investigate the
mechanisms and anatomy that underlie both our ability to attend to
multiple spatial locations simultaneously and the disruption of this
ability in neuropsychological populations.
-
de Haan B, Bither M, Brauer A, Karnath H-O (2015). Neural correlates of
spatial attention and target detection in a
multi-target environment. Cerebral Cortex 25:
2321–2331.
- de Haan B, Stoll T, Karnath H-O (2015). Early sensory processing in right hemispheric stroke patients with and without extinction.Neuropsychologia 73: 141–150.
- de Haan B, Stoll T, Karnath H-O (2015). Early sensory processing in right hemispheric stroke patients with and without extinction.Neuropsychologia 73: 141–150.
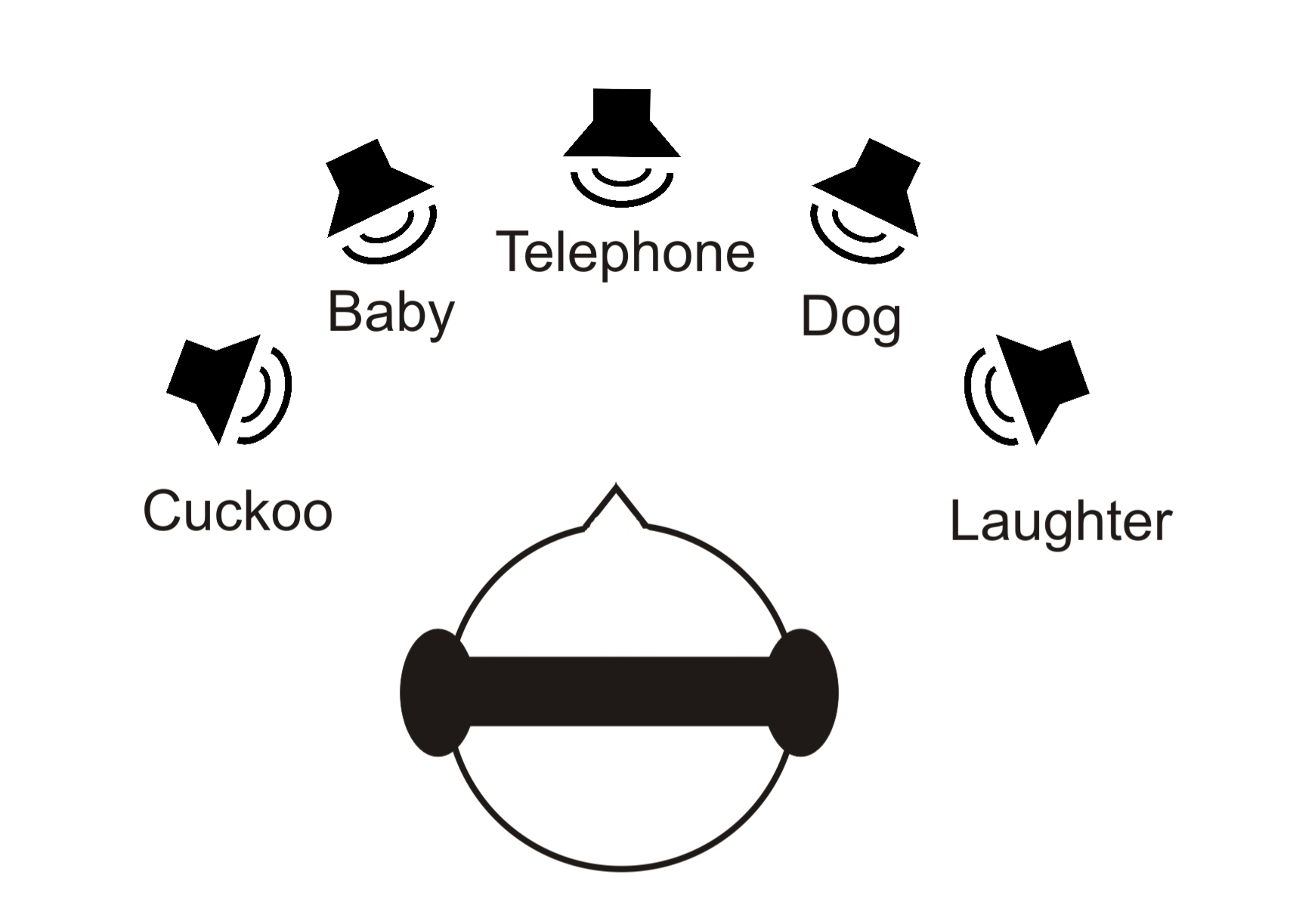
Despite the movements of eyes,
head, and body, a healthy person perceives its environment as a
constant visual and acoustical unit. Humans also show a remarkable
ability to attend to and localise sounds. By means of functional MRI,
we search for the neural correlates underlying these mechanisms.
Likewise, in a soundproof room behavioral studies are carried out to
clarify the mechanisms of auditory localisation in multisound
environments. Our studies are carried out with healthy subjects as well
as stroke patients.
- Zündorf IC, Karnath H-O, Lewald J (2014). The effect of brain lesions on sound localization in complex acoustic environments. Brain 137: 1410-1418.
- Zündorf IC, Lewald J, Karnath H-O (2016). Testing the dual-pathway model for auditory processing in human cortex. NeuroImage 124: 672–681.
- Zündorf IC, Karnath H-O, Lewald J (2014). The effect of brain lesions on sound localization in complex acoustic environments. Brain 137: 1410-1418.
- Zündorf IC, Lewald J, Karnath H-O (2016). Testing the dual-pathway model for auditory processing in human cortex. NeuroImage 124: 672–681.
Stroke patients may exhibit the
peculiar behavior of actively pushing away from the non-hemiparetic
side leading to lateral postural imbalance and a tendency to fall
towards the paralyzed side. This phenomenon has been called the "Pusher
Syndrome". We investigate the cognitive, visual, and vestibular
contributions to understand the mechanism leading to contraversive
pushing.
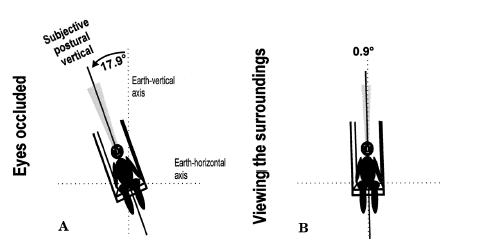
(A) and while viewing their surroundings (B). The patient's SPV shows a marked ipsiversive
deviation from the earth-vertical with occluded eyes.
- Karnath H-O (2007). Pusher syndrome - a frequent but little-known disturbance of body orientation perception. J Neurol 254: 415-24.
- Karnath H-O, Brötz D (2014). Pusher-Syndrom. In: Karnath H-O, Goldenberg G, Ziegler W (eds.) Klinische Neuropsychologie −Kognitive Neurologie. Stuttgart, Thieme, 213-222.
(A) and while viewing their surroundings (B). The patient's SPV shows a marked ipsiversive
deviation from the earth-vertical with occluded eyes.
- Karnath H-O (2007). Pusher syndrome - a frequent but little-known disturbance of body orientation perception. J Neurol 254: 415-24.
- Karnath H-O, Brötz D (2014). Pusher-Syndrom. In: Karnath H-O, Goldenberg G, Ziegler W (eds.) Klinische Neuropsychologie −Kognitive Neurologie. Stuttgart, Thieme, 213-222.
Patients with visual agnosia
cannot recognise
objects in their environment based on visual information. They know
everything about such everyday objects and can even verbally describe
what they should look like. Patients can even provide quite accurate
drawings of typical objects from their memory. Because of their
otherwise intact visual input to the brain, these patients are of
particular interest for research on visual recognition and the usage
and integration of visual information in the human brain. One example
is the influential model on visual information processing that has
suggested a dissociation between action- and perception-related
processing in a dorsal versus ventral stream projection. Appreciating
the enormous impetus of this model we scrutinise some of its basic
assumptions and postulations, investigating visual agnosia.
- Cornelsen S, Rennig J, Himmelbach M (2016). Memory-guided reaching in a patient with visual hemiagnosia. Cortex 79: 32–41.
- Karnath H-O, Rüter J, Mandler A, Himmelbach M (2009). The anatomy of object recognition – visual form agnosia caused by medial occipitotemporal stroke. Journal of Neuroscience
29: 5854-5862.
- Cornelsen S, Rennig J, Himmelbach M (2016). Memory-guided reaching in a patient with visual hemiagnosia. Cortex 79: 32–41.
- Karnath H-O, Rüter J, Mandler A, Himmelbach M (2009). The anatomy of object recognition – visual form agnosia caused by medial occipitotemporal stroke. Journal of Neuroscience
29: 5854-5862.
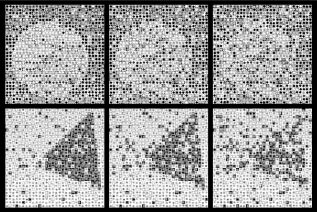
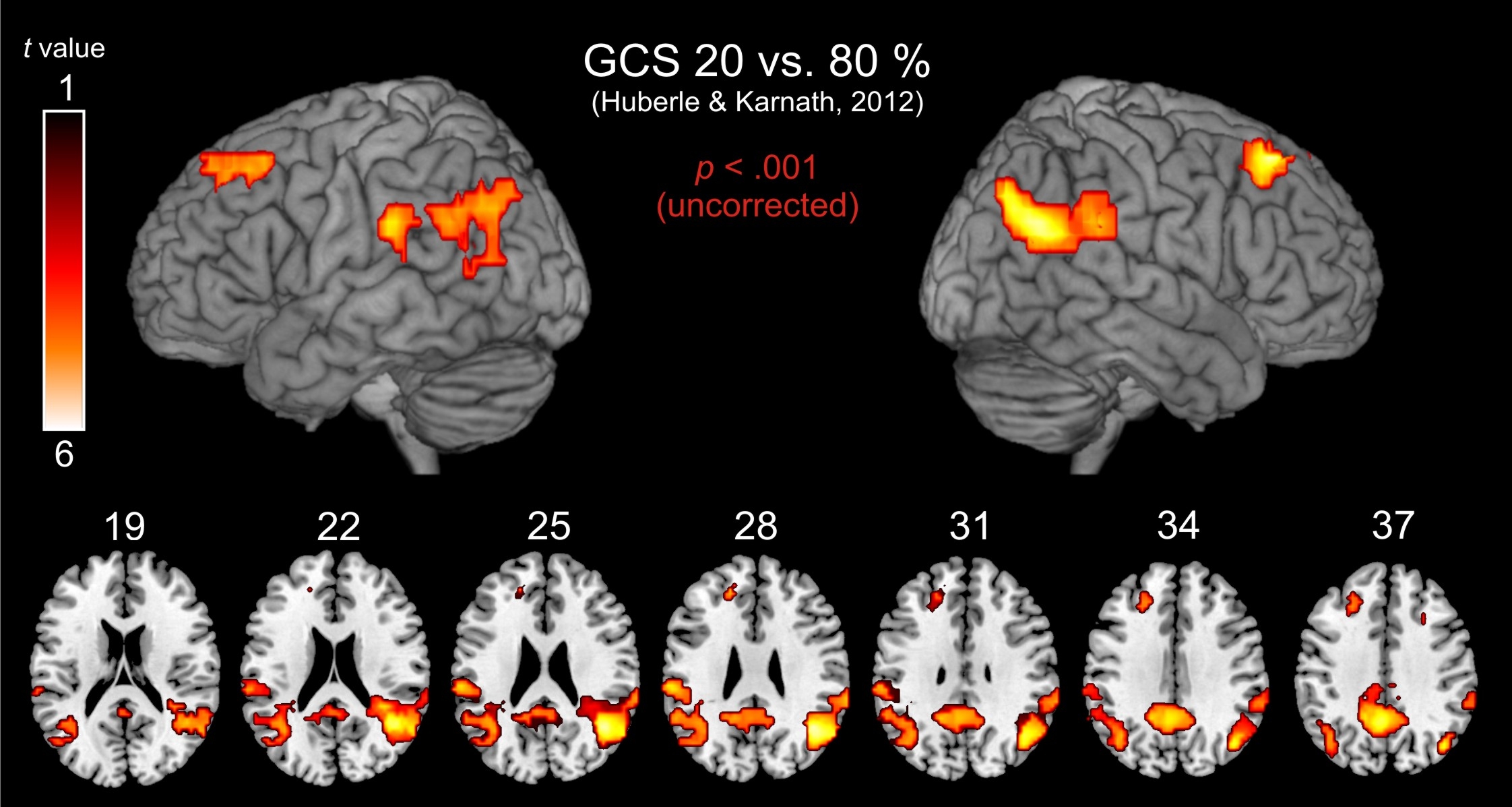
The perception of our
environment not only requires the perception of individual objects, but
also the integration of multiple objects to a global gestalt (e.g. the
integration of individual trees giving rise to the coherent perception
of a forest). A holistic perception of complex visual scenes is a
crucial aspect of human perception. Patients with brain-damage of the
temporo-occipital cortex may show a deficit in global gestalt
perception. This deficit has been termed "simultanagnosia". We
investigate such patients to
reveal the parameters that play a critical role in visual integration
and further improve our understanding of the underlying mechanisms.
Functional neuroimaging of healthy subjects supplements this research,
identifying the role of cortical structures in global Gestalt
perception.
- Balslev D, Odoj B, Rennig J, Karnath H-O (2014). Abnormal center-periphery gradient in spatial attention in simultanagnosia. J Cogn Neurosci 26: 2778-2788.
- Rennig J, Himmelbach M, Huberle E, Karnath H-O (2015). Involvement of the TPJ area in processing of novel global forms. J Cogn Neurosci 27: 1587–1600.
- Balslev D, Odoj B, Rennig J, Karnath H-O (2014). Abnormal center-periphery gradient in spatial attention in simultanagnosia. J Cogn Neurosci 26: 2778-2788.
- Rennig J, Himmelbach M, Huberle E, Karnath H-O (2015). Involvement of the TPJ area in processing of novel global forms. J Cogn Neurosci 27: 1587–1600.
Stroke patients with anosognosia
for
hemiparesis typically are convinced that their limbs function normally
although they have obvious motor defects after stroke. They may
experience the paretic limbs as strange or as not belonging to them, or
even may attribute ownership to another person. Studies suggest that
the insular cortex is integral to self-awareness and to one's beliefs
about the functioning and the ownership of body parts. We evaluate such
phenomena in stroke patients to elucidate the mechanisms leading to
anosognosia, the brain structures typically involved when patients
exhibit this behaviour, as well as its relation to unilateral spatial
neglect.
- Karnath H-O, Baier B (2010). Right insula for our sense of limb ownership and self-awareness of actions. Brain Struct Funct 214: 411-417.
- Baier B, Geber C, Müller-Forell W, Müller N, Dieterich M, Karnath H-O (2015). Anosognosia for obvious visual field defects in stroke patients. Brain Struct Funct 220: 1855-1860.
- Karnath H-O, Baier B (2010). Right insula for our sense of limb ownership and self-awareness of actions. Brain Struct Funct 214: 411-417.
- Baier B, Geber C, Müller-Forell W, Müller N, Dieterich M, Karnath H-O (2015). Anosognosia for obvious visual field defects in stroke patients. Brain Struct Funct 220: 1855-1860.
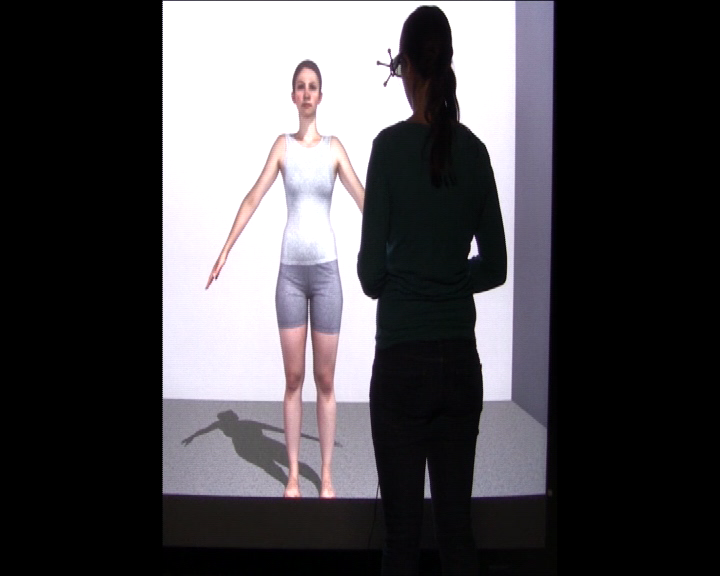
Body size perception is crucial
for our perception of self and also for motion. It is informed by
multiple senses, but as yet, it is unclear how the various sources of
information are processed and combined. Further, little is known about
body size perception in clinical conditions in which body
representation is disturbed. In cooperation with the Dept. of
Psychosomatic Medicine and Psychotherapy (Prof. Giel / Prof. Zipfel),
the Max Planck Institute for Biological Cybernetics (Dr. Mohler / Prof.
Bülthoff) and the Max Planck Institute for Intelligent Systems
(Prof. Black) we investigate body size perception of healthy and
clinical samples in both real world and virtual reality setups.
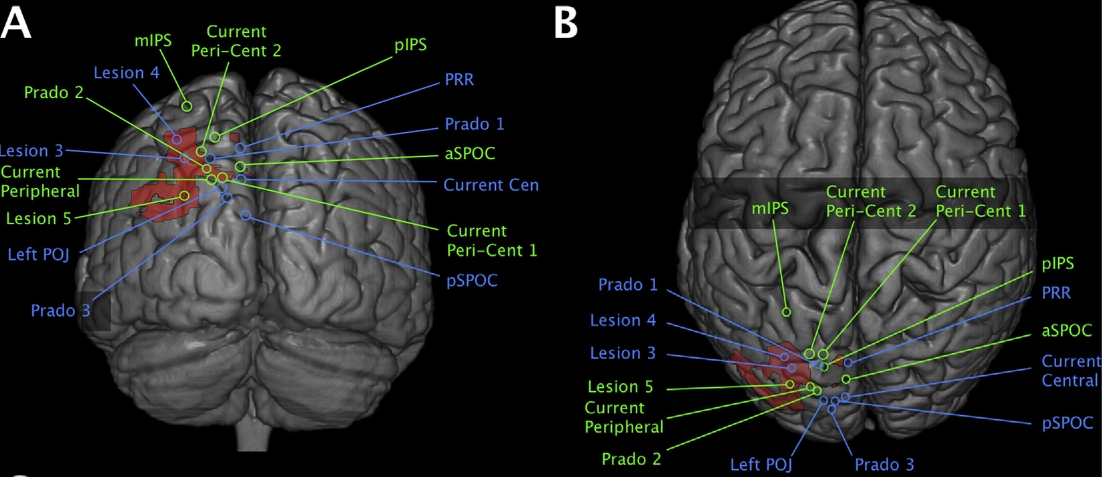
The disorder of optic ataxia,
i.e.
misreaching of visual targets and faulty scaling of hand aperture while
grasping objects, allows for exciting and often surprising insights
regarding the anatomy and functionality of the human sensorimotor
system. The typical characteristics of this impairment together with
its variability in individual patients help us to reveal those cortical
areas and networks that are indispensable for rapid and accurate
visually-guided limb movements and online movement corrections. Despite
its value and importance for the field of action control, research on
optic ataxia is addressed by only a few research groups.
-
Martin JA, Karnath H-O, Himmelbach M (2015). Revisiting the cortical
system for peripheral reaching at the parieto-occipital
junction. Cortex 64: 363-379.
- Borchers S, Müller L, Synofzik M, Himmelbach M (2013). Guidelines and quality measures for the diagnosis of optic ataxia. Frontiers in Human Neuroscience 7: 324.
- Borchers S, Müller L, Synofzik M, Himmelbach M (2013). Guidelines and quality measures for the diagnosis of optic ataxia. Frontiers in Human Neuroscience 7: 324.
Human action control is
characterized by its impressive complexity and flexible adjustment in
tool use and object manipulation. We aim to investigate the cognitive
control mechanisms involved in in these processes, studying both
healthy subjects as well as neurological patients with apraxia. Apraxia
is a common consequence
of vascular
or neurodegenerative defects primarily to the left hemisphere. Apractic
patients have deficits in higher skilled movements independent of
primary motor skills. They lack the
cognitive skills to perform and plan certain actions. Typically
affected skills include imitation of gestures, pantomime of object use,
or solving of mechanical tasks. Our group studies both the cognitive
as well as anatomical basis of this disorder with lesion mapping, fMRI,
and
behavioral studies.

- Goldenberg G, Karnath H-O (2006). The neural basis of imitation is body part specific. Journal of Neuroscience 26: 6282–6287.
- Schell C, Suchan J, Himmelbach M, Haarmeier T, Borchers S (2014). Limb apraxia in acute ischemic stroke: a neglected clinical challenge? Neurocase 20: 158-162.
- Goldenberg G, Karnath H-O (2006). The neural basis of imitation is body part specific. Journal of Neuroscience 26: 6282–6287.
- Schell C, Suchan J, Himmelbach M, Haarmeier T, Borchers S (2014). Limb apraxia in acute ischemic stroke: a neglected clinical challenge? Neurocase 20: 158-162.
Human action control is
characterized by its impressive complexity and flexible adjustment in
tool use and object manipulation. We aim to investigate the cognitive
control mechanisms involved in the evaluation of action affordances
associated with an object and their neuronal correlates. How do we
recognize an usable tool for a particular technical problem? How do
memory and acquired knowledge about tools on the one hand and visual
analysis and deductive reasoning on the other hand contribute to our
respective decision? A small group of brain-damaged patients are
especially impaired in using novel, unfamiliar tools while they are
less impaired in using familiar tools. The examination of such patients
and further behavioral and neuroimaging studies based on observations
in these patients can help us to understand the way different cognitive
sources are combined to come up with a motor behavior that no other
living species can match.
- Belardinelli A, Barabas M, Himmelbach M, Butz M (2016). Anticipatory eye fixations reveal tool knowledge for tool interaction. Experimental Brain Research 234: 2415–2431.
- Belardinelli A, Barabas M, Himmelbach M, Butz M (2016). Anticipatory eye fixations reveal tool knowledge for tool interaction. Experimental Brain Research 234: 2415–2431.
We grasp a screwdriver in a
specific way if we are about to use it and in a very different way if
we just want to put it aside. Despite of such quite obvious
dependencies of visual motor control on object recognition, many
researchers believe that the actual control of human grasping depends
almost entirely on the direct visual information about object sizes
irrespective of any stored knowledge in our memory. In contrast, we
demonstrated that well established associations, build through a
long-term learning process, are powerful enough to change visual motor
control. Interestingly, we also observed some patients with impairments
in the control of grasping who apparently exploited such associations
for an individual improvement: they are better in grasping very
familiar in comparison to neutral geometrical objects. Our work
suggests that the role of object familiarity on the control of
movements was underestimated in the past.
- Borchers S, Verheij R, Smeets JBJ, Himmelbach M (2014). The influence of object height on maximum grip aperture in empirical and modelled data. Journal of Experimental
Psychology: Human Perception and Performance 40: 889-896.
- Borchers S, Himmelbach M (2012). The recognition of everyday objects changes grasp scaling. Vision Research 67: 8-13.
- Borchers S, Verheij R, Smeets JBJ, Himmelbach M (2014). The influence of object height on maximum grip aperture in empirical and modelled data. Journal of Experimental
Psychology: Human Perception and Performance 40: 889-896.
- Borchers S, Himmelbach M (2012). The recognition of everyday objects changes grasp scaling. Vision Research 67: 8-13.
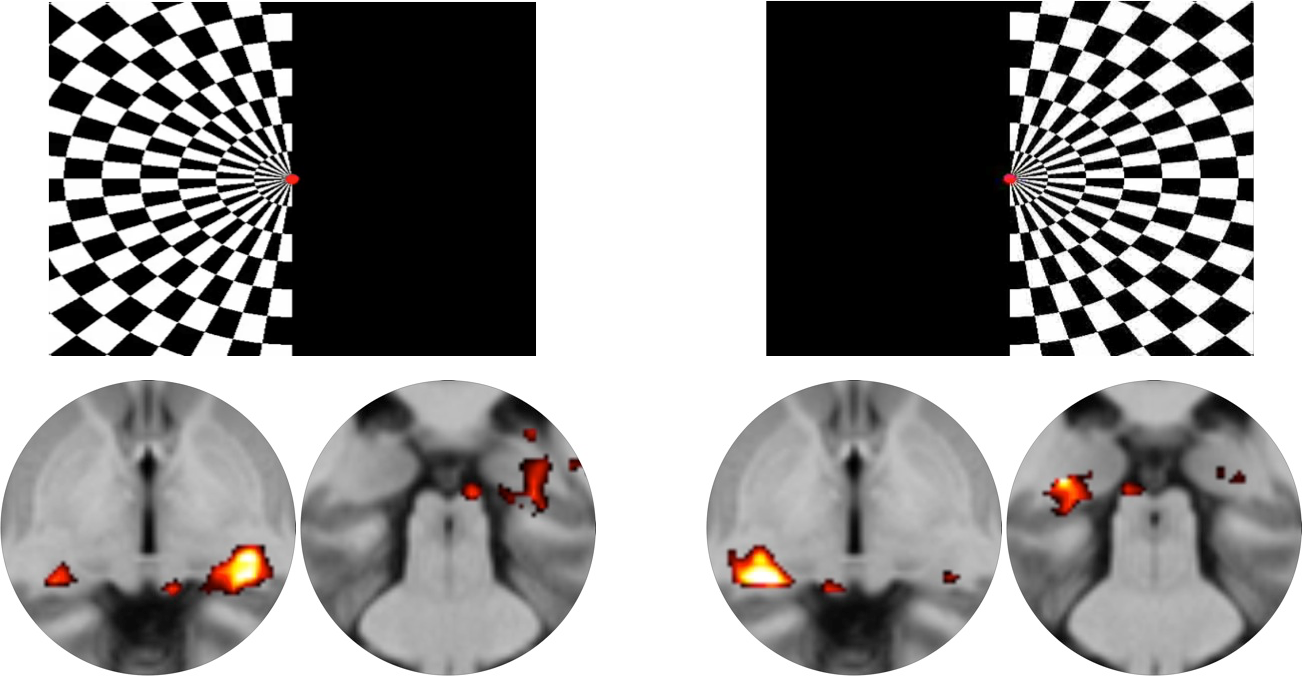
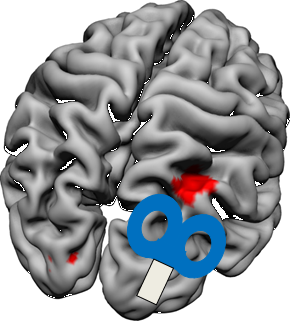
Previous studies have revealed
that the superior colliculi play some role in the execution of arm
movements. However, the precise functional contribution of the
colliculi to the processes of planning and execution and the processing
of a movement’s sensory feedback is still unknown. We explore
this unknown territory by developing experimental designs that allow
for event-related analyses and transfer our paradigms to the ultra-high
field 9.4T scanner at the Max Planck Institute for High-field Magnetic
Resonance (Prof. Scheffler). Using tensor imaging and resting state
fMRI we investigate the connectivity of the superior colliculi within
the sensorimotor network.
- Himmelbach M, Linzenbold W, Ilg UJ (2013). Dissociation of reach-related and visual signals in the human superior colliculus. Neuroimage 82: 61–67.
- Loureiro JR, Hagberg GE, Ethofer T, Erb M, Bause J, Ehses P, Scheffler K, Himmelbach M (2017). Depth-dependence of visual signals in the human superior colliculus at 9.4 T. Human
Brain Mapping 38: 574-587.
- Himmelbach M, Linzenbold W, Ilg UJ (2013). Dissociation of reach-related and visual signals in the human superior colliculus. Neuroimage 82: 61–67.
- Loureiro JR, Hagberg GE, Ethofer T, Erb M, Bause J, Ehses P, Scheffler K, Himmelbach M (2017). Depth-dependence of visual signals in the human superior colliculus at 9.4 T. Human
Brain Mapping 38: 574-587.
We use structural magnetic
resonance imaging methods (T1,T2 FLAIR, DWI) and diffusion tensor
imaging (DTI) to investigate the precise location of brain lesions as
well as the structural connectivity between cortical modules and its
contribution to both intact and impaired brain function. Finally, we
are involved in the development of methodological tools that aid the
(semi)automated segmentation of structural magnetic resonance imaging
data from neuropsychological populations.
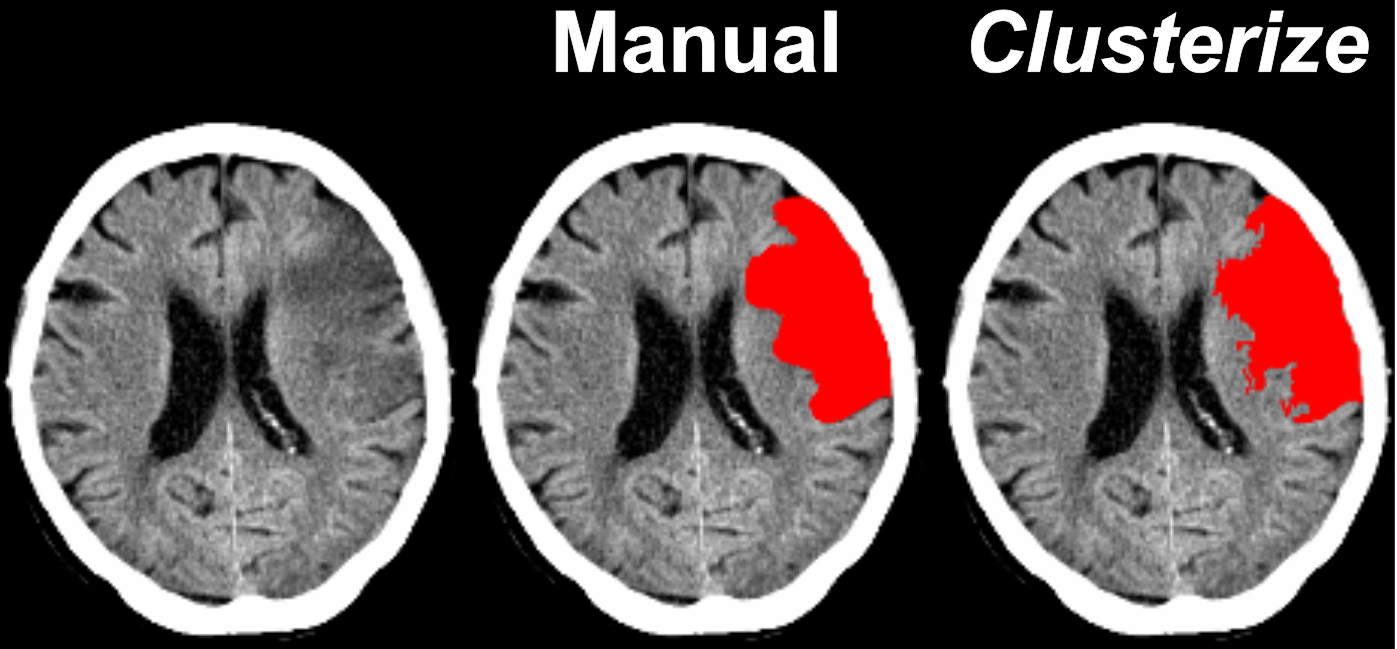
- de Haan B, Clas P, Juenger H, Wilke M, Karnath H-O (2015). Fast semi-automated lesion demarcation in stroke. NeuroImage: Clinical 9: 69–74.
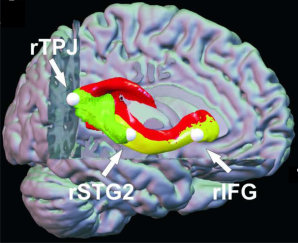
- Suchan J, Umarova R, Schnell S, Himmelbach M, Weiller C, Karnath H-O, Saur D (2014). Fiber pathways connecting cortical areas relevant for spatial orienting and exploration.
Human Brain Mapping 35: 1031-1043.
- de Haan B, Clas P, Juenger H, Wilke M, Karnath H-O (2015). Fast semi-automated lesion demarcation in stroke. NeuroImage: Clinical 9: 69–74.
- Suchan J, Umarova R, Schnell S, Himmelbach M, Weiller C, Karnath H-O, Saur D (2014). Fiber pathways connecting cortical areas relevant for spatial orienting and exploration.
Human Brain Mapping 35: 1031-1043.
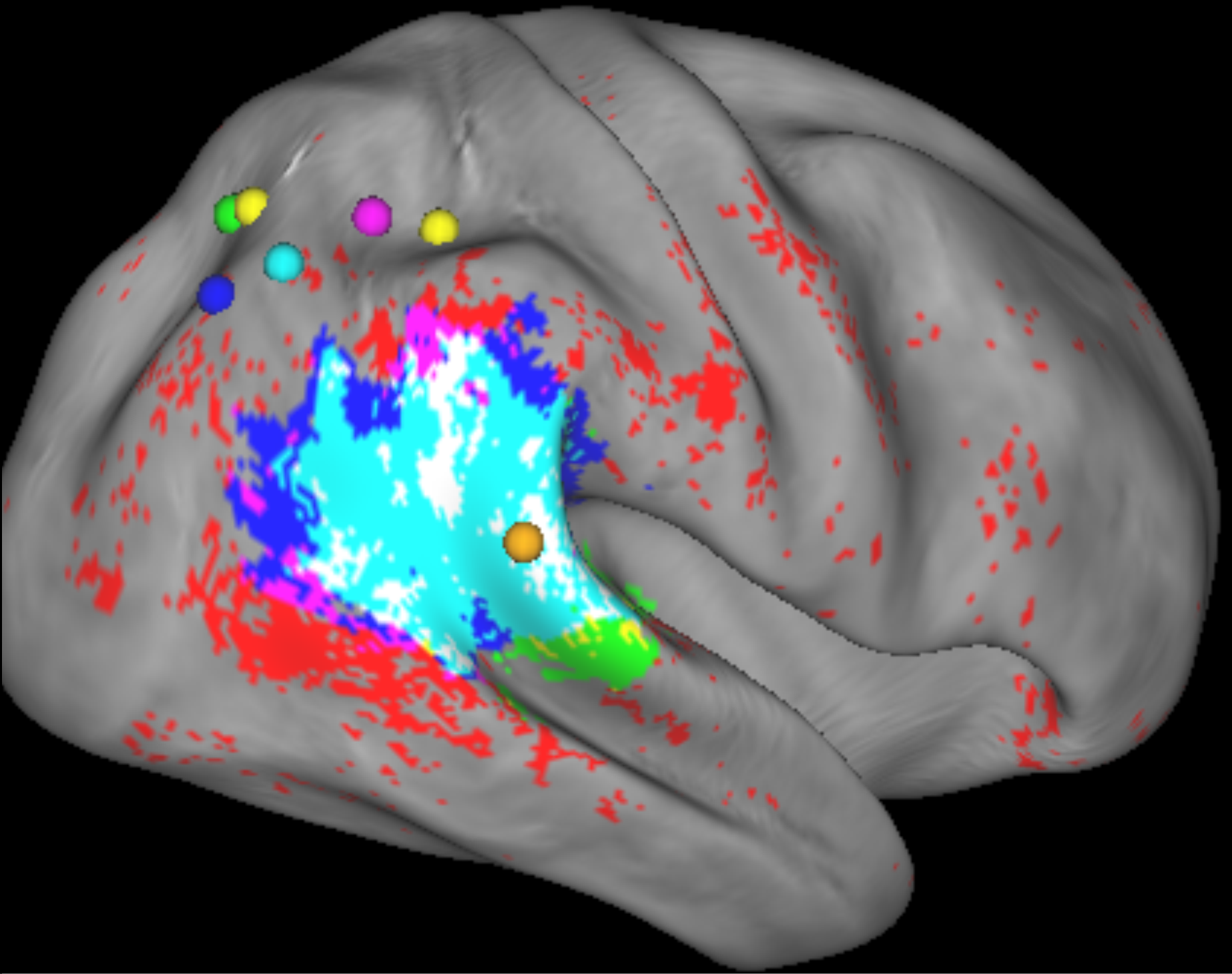
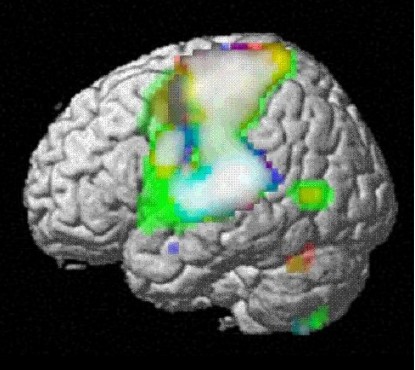
Using diffusion-weighted (DWI),
fluid-attenuated inversion-recovery (FLAIR) magnetic resonance imaging
(MRI) as well as spiral computerized tomography (Spiral-CT) scans we
identify the lesion location(s) typically associated with specific
cognitive disorders. Statistical voxelwise lesion-behaviour mapping
(VLBM) is used to determine relationships between behavioral
measures/disorders and the location of brain injury, revealing the
function of brain regions. Together with Prof. Chris Rorden, University
of South Carolina, we improve and develop new VLBM approaches. We also
use machine learning algorithms in multivariate pattern analysis as an
enhancement to VLBM in the identification of brain networks underlying
behavioral disorders. Beyond the neuroscientific identification of
human brain function, knowledge of critical brain regions for
neurological symptoms can also be used to predict long term post-stroke
outcome and thus can support effective therapeutical planning.
- Smith DV, Clithero J, Rorden C, Karnath H-O (2013). Decoding the anatomical network of spatial attention. PNAS 110: 1518-1523.
- Sperber C, Karnath H-O (2017). Impact of correction factors in human brain lesion-behavior inference. Human Brain Mapping: in press.
- Smith DV, Clithero J, Rorden C, Karnath H-O (2013). Decoding the anatomical network of spatial attention. PNAS 110: 1518-1523.
- Sperber C, Karnath H-O (2017). Impact of correction factors in human brain lesion-behavior inference. Human Brain Mapping: in press.
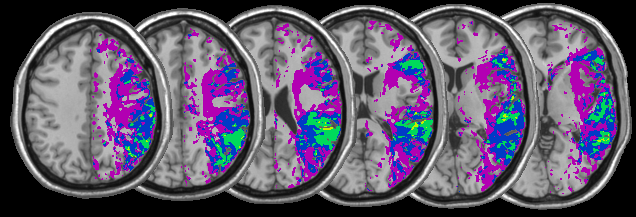
In patients with stroke lesions,
we use PWI to identify the abnormally perfused brain area(s) that
receive enough blood supply to remain structurally intact, but not
enough to function normally. In order to recognize these common areas
in groups of patients, we analyse the increase of time-to-peak (or TTP)
lesion-inducted delays by using spatial normalization of PWI maps as
well as symmetric voxel-wise inter-hemispheric comparisons. These new
techniques allow comparison of the structurally intact but abnormally
perfused areas of different individuals in the same stereotaxic space,
and at the same time avoid problems due to regional perfusion
differences and to possible observer-dependent biases.
- Karnath H-O, Zopf R, Johannsen L, Fruhmann Berger M, Nagele T, Klose U (2005). Normalized perfusion MRI to identify common areas of dysfunction: patients with basal ganglia
neglect. Brain 128: 2462-2469.
- Zopf R, Klose U, Karnath H-O (2012). Evaluation of methods for detecting perfusion abnormalities after stroke in dysfunctional brain regions. Brain Struct Funct 217: 667-675.
- Karnath H-O, Zopf R, Johannsen L, Fruhmann Berger M, Nagele T, Klose U (2005). Normalized perfusion MRI to identify common areas of dysfunction: patients with basal ganglia
neglect. Brain 128: 2462-2469.
- Zopf R, Klose U, Karnath H-O (2012). Evaluation of methods for detecting perfusion abnormalities after stroke in dysfunctional brain regions. Brain Struct Funct 217: 667-675.
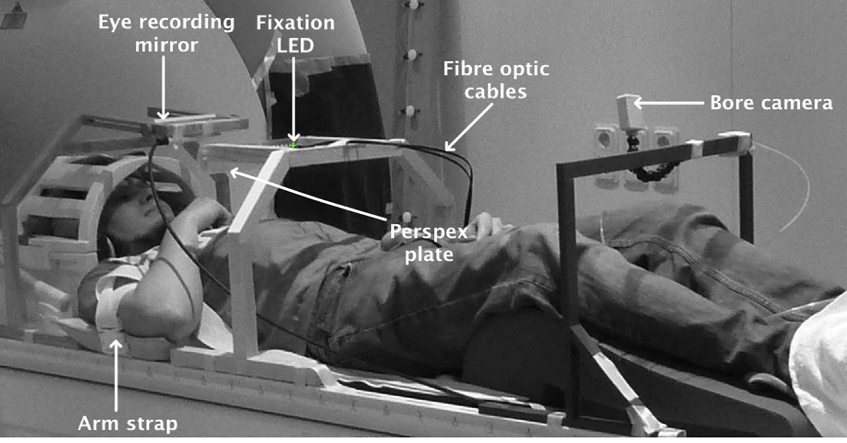
fMRI allows to study brain
activity in the
intact human brain across its whole volume. Most of our fMRI projects
are conducted at a 3T Siemens Prisma system located at the University
Hospital Tübingen in collaboration with the Department for
Biomedial Magnetic Resonance. The available equipment comprises diverse
setups for stimulus presentation and response collection including
mutliple state-of-the-art eye eye tracker systems, auditory stimulation
systems, and MR-compatible video cameras for motion tracking and
qualitative observations of participants’ behaviour and
performance. Beyond 3T imaging we conduct experiments at the 9.4T
Siemens Scanner (see below) in cooperation with the Max Planck
Institute for Biological Cybernetics.
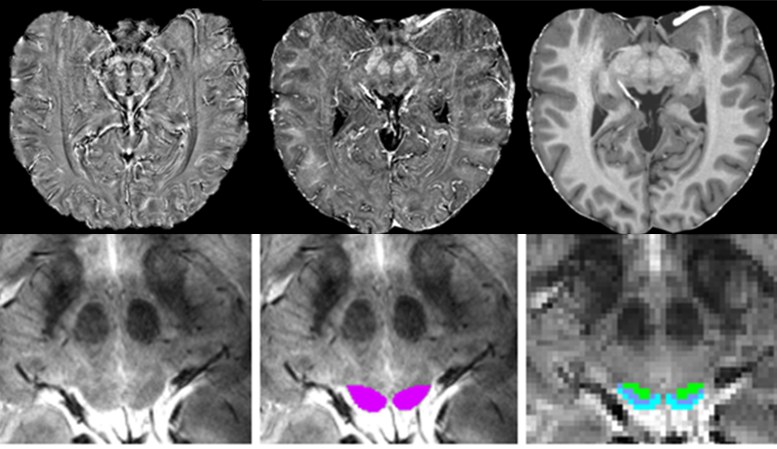
In cooperation with the Max
Planck Institute for Biological Cybernetics (Prof. Scheffler) we are
exploiting the potential of Ultra High-Field Magnetic Resonance imaging
for submillimetre fMRI. The MR system has a field strength of 9.4 Tesla
and a usable volume of 60 cm diameter for human studies. The current
focus of our research addresses the functional organisation of the
human superior colliculi. We aim to establish anatomical sequences that
allow us to identify brainstem nuclei with isotropic submillimeter
resolution; establish functional sequences to acquire blood oxygen
level dependent (BOLD) signals with isotropic submillimeter resolution;
and detect BOLD signals to clarify the precise functional contribution
of the colliculi to the processes of planning and execution and the
processing of a movement’s sensory feedback.
- Loureiro JR, Himmelbach M, Ethofer T, Pohmann R, Martin P, Bause J, Scheffler K, Grodd W, Hagberg G (2018). In-vivo quantitative structural imaging of the human midbrain and the
superior colliculus at 9.4T. Neuroimage 177: 117-128.
- Loureiro JR, Hagberg GE, Ethofer T, Erb M, Bause J, Ehses P, Scheffler K, Himmelbach M (2017). Depth-dependence of visual signals in the human superior colliculus at 9.4 T. Human
Brain Mapping 38: 574-587.
- Loureiro JR, Himmelbach M, Ethofer T, Pohmann R, Martin P, Bause J, Scheffler K, Grodd W, Hagberg G (2018). In-vivo quantitative structural imaging of the human midbrain and the
superior colliculus at 9.4T. Neuroimage 177: 117-128.
- Loureiro JR, Hagberg GE, Ethofer T, Erb M, Bause J, Ehses P, Scheffler K, Himmelbach M (2017). Depth-dependence of visual signals in the human superior colliculus at 9.4 T. Human
Brain Mapping 38: 574-587.
Transcranial magnetic
stimulation (TMS) briefly disrupts ongoing neural processing in a small
part of the brain and so can be used to induce a so-called virtual
lesion in healthy subjects. This allows us to determine where in the
brain neural activity is causally connected to task performance at an
excellent temporal and spatial resolution. We use TMS to complement our
lesion analysis and fMRI studies and so obtain a more detailed view of
the functional architecture of the brain.
-
Ritzinger B, Huberle E, Karnath H-O (2012). Bilateral theta-burst TMS
to influence global Gestalt perception. PLoS ONE 7: e47820.
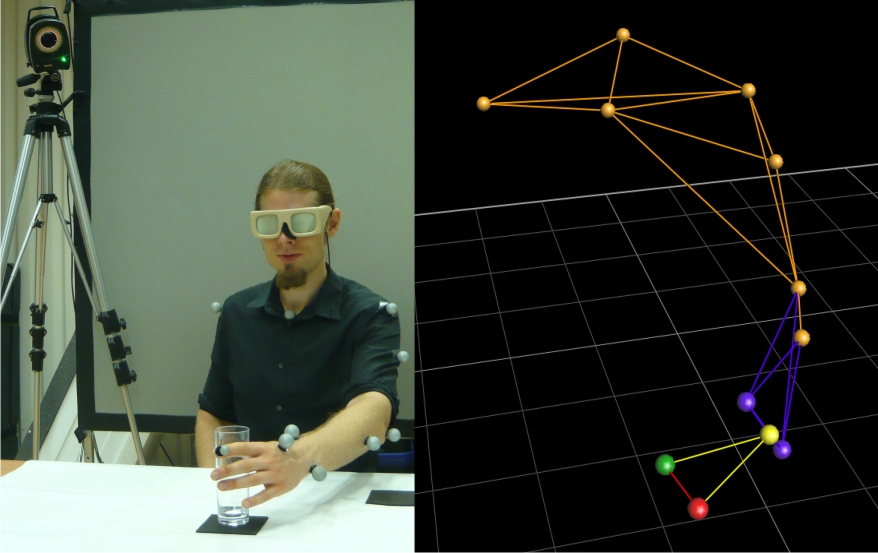
The human brain comprises
complex networks to perform action such as grasping, pointing, or
object use. These skills can be affected in stroke patients, e.g.
patients suffering from optic ataxia or apraxia. To study the human
action system, our group uses motion capturing in healthy subjects and
neurological patients. VICON Motion Capture Systems can record the
position of reflective markers attached to the body or the hand and
track movements with high temporal resolution. As the motion capture
system does not inhibit subjects with cables, we are also able to study
natural movements.
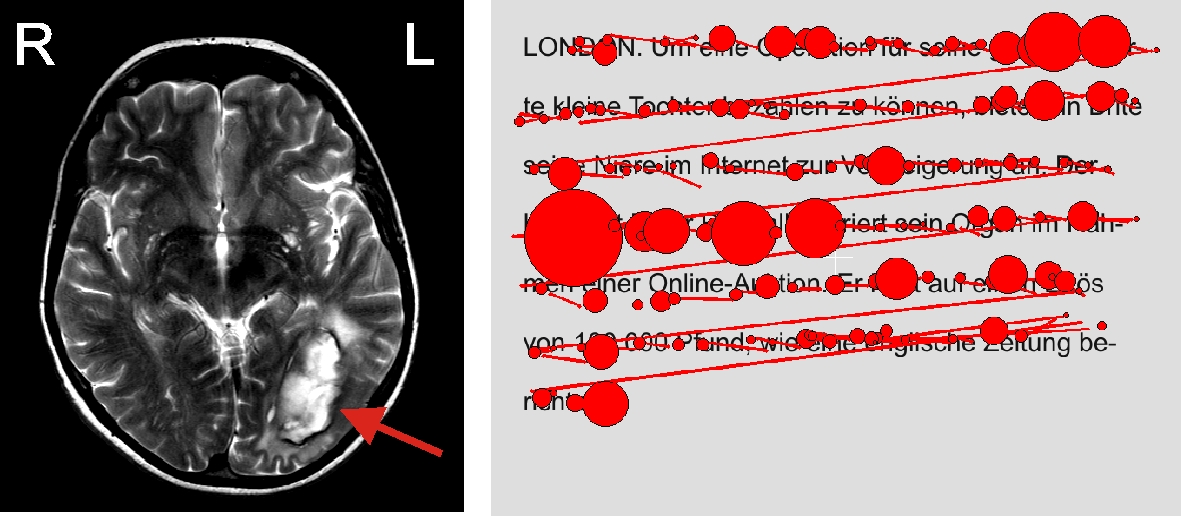
Our video- and coil-based eye
tracking systems allow us to monitor eye movements in both healthy
subjects and neurological patients at an excellent temporal and spatial
resolution. We use this eye tracking data to make inferences about
healthy and pathological attentional processes as well as to monitor
fixation during task performance.
-
Belardinelli A, Barabas M, Himmelbach M, Butz M (2016). Anticipatory
eye fixations reveal tool knowledge for tool interaction.
Experimental Brain Research 234: 2415–2431.
Immersive virtual reality (VR)
allows us to overcome limitations of other approaches and to enhance
ecological validity of experimental setups. For example, it enables us
to expose participants to a mirror image or even first person
perspective of their own visually manipulated body. Together with our
collaboration partners at the Max Planck Institute for Biologial
Cybernetics we are using portable VR setups that are displayed via a
headmounted display (Oculus DK-2) and therefore allow for bedside
testing.
